ANGINA PECTORIS:
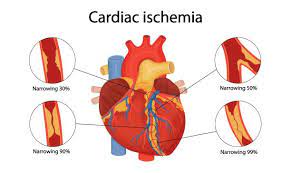
Angina pectoris is a clinical pattern of Ischemic heart disease( IHD) performing from flash myocardial ischaemia if the heart muscle doesn’t get as important blood as it needs. This generally happens because one or further of the heart’s arteries is narrowed or blocked. It’s characterised by paroxysmal pain in the sub sternal or precordial region of the casket which is exacerbated by an increase in the demand of the heart and relived by a drop in the work of hear. Frequently, the pain may radiates towards the left arm, neck jaw or right arm.
TYPES OF ANGINA PECTORIS:
There are mainly three types of clinical patterns of angina pectoris is noticed with some difference in their pathogenesis.
1. Stable angina (common form): Also called as typical angina. In this type of angina pectoris there is a deposition of atherosclerosis plaques in the coronary arteries. It result. Harrowing of the lumen of the arteries whenever, demand of the heart increases such Lack of exercise emotional reactions, the pain for angina develops. This is because The coronary arteries cannot supply enough b due to reduced lumen size.
2. Variant angina (uncommon form): In this case, there is transient vasospasm of the coronary arteries. It will result in decreased blood flow to the heart. The demand of heart is not changed, but because blood supply. Has reduced, so there will be anginal pain. Attacks occur at rest or during sleep and are unpredictable.
3. Unstable angina: In this case, there are atherosclerosis plaques will supposition in arteries These and will block the coronary arteries. There is also a vasospasm of the coronary arteries. So combination of both atherosclerotic plaques and vaso constriction of blood vessels will decrease blood flow to the heart. It will then lead to development of angina. Chronically, reduced blood supply of cardiac muscle causes atrophy of cardiac muscle fibrosis replacement. Reduced in myocardial work capacity leads to CHF and may damage the tissue to produce unstable cardiac arrhythmia.
ANGINA PECTORIS SYMPTOMS:
The most prominent symptom of angina Is pain or pressure in the casket. It may feel like squeezing or wholeness in the middle of the casket and it can radiate outward to the neck, jaw, shoulder, back or arms. With stable angina, occurrences of pain are regular circumstance and come a predictable as triggers are linked. It typically lasts lower than five twinkles and goes down with rest and/ or drug.
With unstable angina, the pain is different from that endured with stable angina and isn’t predictable. It’s sharper, unanticipated( no detector has been linked), and doesn’t go down with rest or drug. Variant angina causes sharp bursts of pain, frequently in the middle of the night. They can last upto 30 twinkles but may respond to drug. Other symptoms can include impassiveness or chinking, anxiety, fainting, dizziness, sweating, briefness of breath, pale skin, irregular twinkle, nausea or fatigue.
PREVENTION OF ANGINA PECTORIS:
• Maintain proper diet charts and avoid the intake of fat rich food. Fat is the main
factor which increases the levels of lipids in blood so, it is necessary to avoid
saturated fat in order to prevent arteriosclerosis.
• Avoid smoking
• Take proper test
• Lifestyle changes
• Adequate physical exercise is essential
• Level of cholesterol and hypertension should be monitored
TREATMENT OF ISCHEMIC HEART DISEASE:
1. Medications:
• Organic Nitrates: This stimulates the intracellular cyclic- GMP, which results in
vascular smooth muscle relaxation of both arterial and venous vasculature.e.g.
Isosorbide dinitrate.
• B- Blockers: B- Blockers act by reducing cardiac work and 02 consumption.e.g.
Propranolol, Atenolol.
• Calcium Channel Blockers: Calcium antagonist inhibits the passage of calcium ions through voltage-dependent L-type calcium channels in cell membranes in the heart and vascular smooth muscle as well as some other hyperexcitable apkins.e.g. Amlodipine Nifedipine.
• Statins: Statins are used to reduce the cholesterol situations in hyperactive
cholesterolemia. Statins are the HMG-CoA reductase impediments.e.g. Atorvastatin,
Rusvastatin.
2. Angioplasty and stent placement: Angioplasty is nothing but a procedure in which a small device is inserted into narrowed blood vessels that supply the required amount of blood to the heart. This device widens the arteries and increases the flow of blood. Balloon angioplasty is also called as PTCA(coronary percutaneous transluminal angioplasty). It uses a thin small tube called a catheter and has a tiny balloon at its tip of the catheter.
The tube which is inserted into the blood stream by using a large vessel in the arm or leg. By watching the progress of the tiny tube on an X-ray, the cardiologist will monitor or guide the tube into the heart, where it is inserted into a narrowed coronary artery. The tiny balloon is then inflated to widen the narrowed area. During most of these procedures, cardiologists also insert a metal wire frame that serves as a scaffolding to help keep the artery open. This device is called a stent. The stent will prevent the closing of arteries when it placed. There are mainly two types of stents:
• Bare metal stents
• Drug coated stents
3. Bypass surgery: In this bypass type of surgery, a graft bypass may be created by using a vessel from another part of body or a tube which is made up of synthetic fabric. This will allows complete blood flow around the narrowed or blocked artery.